As we all know somalis are stereotyped for having a fat bum and weird looking knees i took the time to research these stereotypes and what i found out is that they are physical deformities known as Lordosis and knock knees.
Lordosis
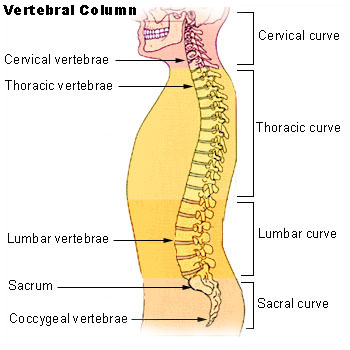
Lordosis is historically defined as an
abnormal inward curvature of the lumbar spine.
[1] [2] However, the terms
lordosis and
lordotic are also used to refer to the normal inward curvature of the
lumbar and
cervical regions of the human
spine.
[3] Similarly,
kyphosis historically refers to
abnormal convex curvature of the spine. The normal outward (convex) curvature in the
thoracic and
sacral regions is also termed
kyphosis or
kyphotic. The term comes from the Greek lordōsis, from
lordos ("bent backward").
[4]
Lordosis in the
human spine makes it easier for humans to bring the bulk of their mass over the
pelvis. This allows for a much more efficient walking
gait than that of other
primates, whose inflexible spines cause them to resort to an inefficient forward leaning "bent-knee, bent-waist" gait. As such, lordosis in the human spine is considered one of the primary physiological adaptations of the human skeleton that allows for human gait to be as energetically efficient as it is.
[5]
Measurement and diagnosis of lumbar hyperlordosis can be difficult. Obliteration of vertebral end-plate landmarks by interbody fusion may make the traditional measurement of segmental lumbar lordosis more difficult. Because the L4–L5 and L5–S1 levels are most commonly involved in fusion procedures, or arthrodesis, and contribute to normal lumbar lordosis, it is helpful to identify a reproducible and accurate means of measuring segmental lordosis at these levels.
[15][16] A visible sign of hyperlordosis is an abnormally large arch of the lower back and the person appears to be puffing out his or her stomach and buttocks.
Precise diagnosis is done by looking at a complete medical history, physical examination and other tests of the patient.
X-rays are used to measure the lumbar curvature. On a lateral X-ray, a normal range of the lordotic curvature of between 20° and 60° has been proposed by Stagnara et al., as measured from the inferior endplate of
Th12 to the inferior endplate of
L5.
[17] The Scoliosis Research Society has proposed a range of 40° and 60° as measured between the upper endplate of Th12 and the upper endplate of S1.
[17] Individual studies, although using other reference points, have found normal ranges up to approximately 85°.
[17] It is generally more pronounced in females.
[17] It is relatively constant through adolescence and young adulthood, but decreases in the elderly.
[17]
Treatment[edit]
Exercises[edit]
Some corrective exercises can be done to alleviate this issue, it may take several months to fix (provided that the person sits less, stands with a neutral pelvis and sleeps on their back).
Since lumbar hyperlordosis is usually caused by habitual poor posture, rather than by an inherent physical defect like
scoliosis or
hyperkyphosis, it can be reversed.
[6] This can be accomplished by stretching the lower back, hip-flexors, quads and strengthening the abdominal muscles, hamstrings and glutes.[
citation needed] Strengthening the gluteal complex is a commonly accepted practice to reverse excessive lumbar lordosis, as an increase in gluteals muscle tone assist in the reduction excessive anterior pelvic tilt and lumbar hyperlordosis.
[19] Local intra-articular hip pain has been shown to inhibit gluteal contraction potential,
[20] meaning that hip pain could be a main contributing factor to gluteal inhibition. Dancers should ensure that they don't strain themselves during dance rehearsals and performances. To help with lifts, the concept of isometric contraction, during which the length of muscle remains the same during contraction, is important for stability and posture.
[21]
Lumbar hyperlordosis may be treated by strengthening the hip extensors on the back of the thighs, and by stretching the hip flexors on the front of the thighs.
Only the muscles on the front and on the back of the thighs can rotate the pelvis forward or backward while in a standing position because they can discharge the force on the ground through the legs and feet. Abdominal muscles and erector spinae can't discharge force on an anchor point while standing, unless one is holding his hands somewhere, hence their function will be to flex or extend the torso, not the hip[
citation needed]. Back hyper-extensions on a
Roman chair or inflatable ball will strengthen all the
posterior chain and will treat hyperlordosis. So too will stiff legged deadlifts and supine hip lifts and any other similar movement strengthening the posterior chain
without involving the hip flexors in the front of the thighs. Abdominal exercises could be avoided altogether if they stimulate too much the psoas and the other hip flexors.
Controversy regarding the degree to which manipulative therapy can help a patient still exists. If therapeutic measures reduce symptoms, but not the measurable degree of lordotic curvature, this could be viewed as a successful outcome of treatment, though based solely on subjective data. The presence of measurable abnormality does not automatically equate with a level of reported symptoms.
[22]